컨텐츠 내용을 수정할 수 있습니다
Sulfonamides
Uricostatics (allopurinol)
Lamotrigine
Phenytoins
Antibiotics (penicillins, quinolones)
| Condition | BSA Involvement | Mucous Membranes | Key Distinguisher |
|---|---|---|---|
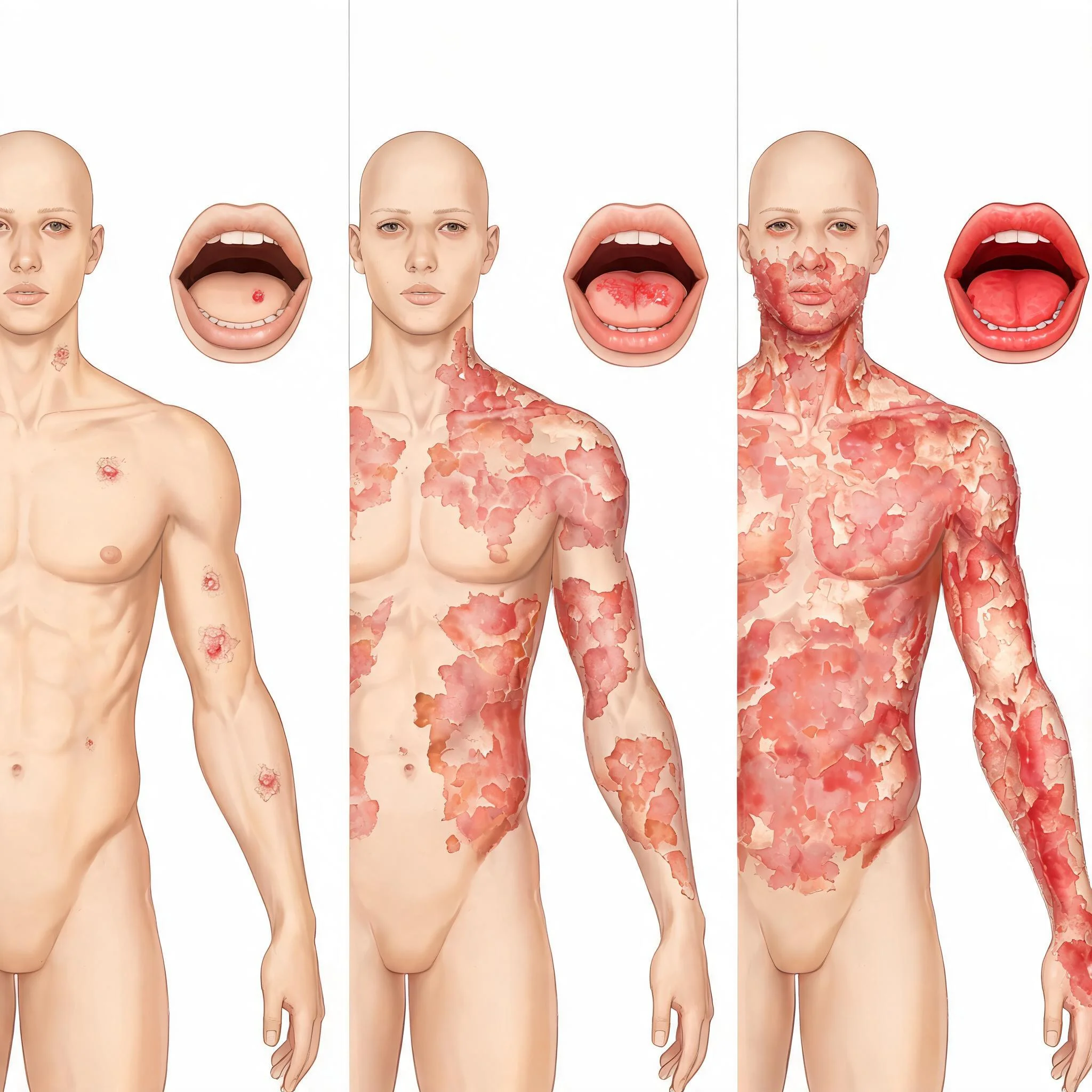
| Stevens-Johnson Syndrome | <10% | Always involved | Target lesions + mucosal erosions |
| Toxic Epidermal Necrolysis | >30% | Always involved | Widespread sheet-like detachment |
| Erythema Multiforme | <10% | Minimal/absent | Target lesions without mucosal involvement |
| Drug Rash | Variable | Rarely involved | No target lesions or detachment |
A 45-year-old patient presents with fever, painful mouth sores, and target-like skin lesions covering 8% of body surface area. History reveals starting trimethoprim-sulfamethoxazole 5 days ago for UTI. Priority action: Discontinue antibiotic immediately and prepare for intensive monitoring.
Stop the offending drug
Target lesions present
Eyes need protection
Vital signs monitoring
Electrolyte balance
Nikolsky's sign positive
Sepsis prevention priority
다음 이론을 계속 학습하려면 로그인하세요.
로그인하고 계속 학습필기노트, 하이라이터, 메모는 잘 쓰고 있어?
내보내줘운영진이 검토할게요!
마이페이지에서 차단한 회원을 관리할 수 있어요.